tree in bud opacities pneumonia
The purpose of this study was to determine the relative frequency of. Tree-in-bud opacities.

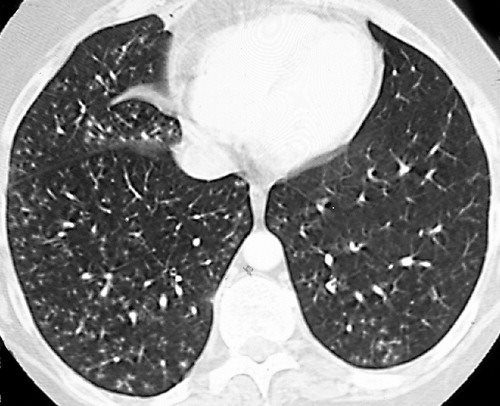
Chest Ct With Multifocal Tree In Bud Opacities Diffuse Bronchiectasis Download Scientific Diagram
Similarly chronic eosinophilic pneumonia typically results in consolidation mainly in the peripheral lung regions but it may.

. Intravascular pulmonary tumor embolism often occurs in cancers of the breast liver kidney stomach prostate and ovaries and can lead to the tree-in-bud sign in HRCT 214. Tree-in-bud TIB opacities are a common imaging finding on thoracic CT scan. When abnormal imaging will most often appear as a bronchiolitis tree-in-bud opacities on CT or subtle perivascular interstitial opacities on chest radiographs a bronchopneumonia tree-in-bud opacities and patchy regions of consolidation on CT or multifocal areas of consolidation on chest radiographs or as multifocal pneumonia multifocal.
Tree-In-Bud Pattern A lymphoid interstitial infiltrate in the walls of the small airways follicular bronchiolitis may cause small centrilobular nodules and the tree-in-bud pattern Fig. Infectious bronchiolitis is by far the most common type of bronchiolitis and can be classified according to its clinical. However to our knowledge the relative frequencies of the causes have not been evaluated.
Often seen as tree-in-bud opacities bronchial wall thicken-ing bronchiolar dilatation often referred to as bronchiolecta-sis and mosaic attenuation andor air trapping if expiratory imaging is used. More extensive lympho - cytic infiltrations may be associated with lymphoid interstitial pneumonia LIP with ground-. Organizing pneumonia most commonly results in a patchy bilateral consolidation that has a predominantly peribronchial and peripheral distribution on CT but it occasionally may be diffuse.
1012 Poorly defined centrilobular nodules associated with branching linear and nodular opacities ie tree-in-bud sign are the typical HRCT findings of infective bronchiolitis frequently. We here describe an unusual cause of TIB during the COVID-19 pandemic. Note the scattered lung nodules surrounded by.
These small clustered branching and nodular opacities represent terminal airway mucous impaction with adjacent peribronchiolar inflammation. The tree-in-bud sign is a nonspecific imaging finding that implies impaction within bronchioles the smallest airway passages in the lung. It is either caused by the filling of the centrilobular arteries with tumour emboli or by the fibrocellular intimal hyperplasia induced by tumour microemboli.
It is most commonly associated with infectious diseases affecting the bronchioles1 OP resulting in a tree in bud pattern has been previously suggested2 However a clear radiological-pathological correlation of OP filling the bronchioles resulting in a tree in bud pattern has to the best of our knowledge not yet been clearly demonstrated. Although initially described in 1993 as a thin-section chest CT finding in active tuberculosis TIB opacities are by. Tree-in-bud refers to a pattern seen on thin-section chest CT in which centrilobular bronchial dilatation and filling by mucus pus or fluid resembles a budding tree.
The disease presented pathologically with exogenous lipoid pneumonia poorly formed granulomas and foreign bodytype multinucleated giant cells with or without foreign material. Thin-section CT scan shows peripheral poorly defined centrilobular nodules and tree-in-bud opacities bilaterally. While the tree-in-bud appearance usually represents an endobronchial spread of infection given the proximity of small pulmonary arteries and small airways sharing branching morphology in the bronchovascular bundle a rarer cause of the tree-in-bud sign is infiltration of the small pulmonary arteriesarterioles or.
I do not believe that the CT findings of COVlD-19 are pathognomonic or different from other causes of acute lung injury. A young male patient who had a history of fever cough and respiratory distress presented in the emergency department. In the acute phase bacterial pneumonia manifests in the form of segmental or lobar consolidation Fig 2 possibly with cavitation and related hilar and mediastinal adenopathies.
Tib opacities are also associated with bronchiectasis and small airways obliteration resulting in mosaic air trapping. Metastastatic tumour emboli in pulmonary arterioles may also present with a tree-in-bud pattern which in this case refers to the vascular rather than the bronchial tree. Multiple causes for tree-in-bud TIB opacities have been reported.
Malignancy can be associated with the tree-in-bud sign. The radiologic presentation was typically one of multilobar centrilobular nodularity tree-in-bud and airway thickening with a subset of patients having evidence of fibrosis. Subsequently question is what causes tree in bud opacities.
Jennifer hong ba francisca zuazo md hanyuan shi md 1 1 tulane university la new orleans. This is the classic appearance of the tree in bud pattern seen on chest ct. Tree-in-bud TIB appearance in computed tomography CT chest is most commonly a manifestation of infection.
Usually somewhat nodular in appearance the tree-in-bud pattern is generally most pronounced in the lung periphery and associated with abnormalities of the larger airways. Are tree-in-bud nodules cancerous. Aspiration Pneumonia and Tree in Bud Sign 87 year old male with history of cough and suspicion of aspiration shows barium aspiration into the proximal trachea upper right The scout view upper right shows an infiltrate at the right base Thickened airways in the right lower lobe 2nd row left is associated with a pneumonic infiltrate in the right lower lobe lower right.
Please remember this important caveat though. Radiologic features of tree-in-bud opacities can suggest MTC infection but includes other differentials such as aspiration viral or other bacterial infection. Pneumonia due to respiratory syncytial virus in a 23-year-old man with leukemia.
Since the initial report of endobronchial spread of pulmonary tuberculosis the tree-in-bud sign has been reported in a wide variety of health conditions including infectious diseases aspiration pneumonia congenital disorders idiopathic disorders inhalation immunologic disorders connective disorders 23456 and central lung cancer involving the. Clinical differentiation of MTC necrotizing pneumonia from the other bacterial causes is difficult because there is no pathognomonic feature for either. Causes for TIB opacities were established in 166.
TIB opacities represent a normally invisible branches of the bronchiole tree 1 mm in diameter that are severely impacted with mucous pus or fluid with resultant dilatation and budding of the terminal bronchioles 2 mm in diameter1 photo. The differential for this finding includes malignant and inflammatory etiologies either infectious or sterile. The purpose of this study was to determine the relative frequency of causes of TIB opacities and identify patterns of disease associated with TIB opacities.

Pdf Tree In Bud Semantic Scholar
2

Tree In Bud Caused By Haemophilus Influenzae Radiology Case Radiopaedia Org

References In Causes And Imaging Patterns Of Tree In Bud Opacities Chest
2
Tree In Bud Sign Lungs
Afmr Tree In Bud Appearance On Ct Scan Of Chest
2
View Of Tree In Bud The Southwest Respiratory And Critical Care Chronicles